
ISSN (0970-2083)
ISSN (0970-2083)
Bina Rani1, Aditi Trivedi2, Raj Kumar Pathak3 and Raaz K. Maheshwari4*
1Department of Engineering Chemistry & Environmental Engineering, Poornima College Engineering, Sitapura, Jaipur 302 022, Rajasthan, India
2Vyom Labs. ( IT Service Management Solutions Company), Baner, Pune 411 045, M.S., India
3Department of Biotechnology, P.G. Thadomal Shahani Engineering College, Bandra, Mumbai 400 050, M.S. India
4Department of Chemistry, Sh Baldev Ram Mirdha Govt. P.G. College, Nagaur 341 001, Rajasthan, India
Received date: 04 September, 2013; Accepted date: 10 October, 2013
Visit for more related articles at Journal of Industrial Pollution Control
Excessive concentration of fluoride in drinking water has deleterious effects on human health and causes fluorosis which progresses gradually and becomes a crippling malady in the long run. It affects young, old, poor, rich, rural, and urban population and has attained a very alarming dimension. The Rajasthan state has extreme climatic and geographical condition due to which it suffers of both the problems- quantity and quality of water. In most part of the state groundwater is either saline or having high nitrates and fluoride content. Groundwater is the major source of drinking water and amounts to be over 94% of the drinking water demand. Groundwater and its level is deeper year-byyear due to over exploitation. As the water table is receding more and more water sources are becoming prone to higher fluoride concentration. The pattern and prevalence of fluorosis in human population are determined by a number of epidemiological factors like water chemistry, demographic and nutritional profile of the community and high mean annual temperature of the area. Alum is used as the coagulant in the treatment process. It has several disadvantages like high sludge volume, residual aluminium, wearing effects on the treatment structure. Therefore, an alternative to alum for defluoridation assumes importance. Although number of defluoridation methods are available, but the Nalgonda Technique has been mostly adopted in Indian context. The main problem of the Nalgonda Technique is the residual Aluminium in treated water which at times is found to be higher than the permissible limit, i.e. 0.2mg/L. In present study we aim to reduce the use of Alum by bringing down the fluoride level firstly with Moringa oleifera (MO) seeds powder and then using Alum later on. For reduction from low fluoride levels less Alum will be required as compared to reduction from high fluoride levels and hence, we would be able to reduce the residual aluminium in the treated water. Apart from solving the residual aluminium problem, coagulation by MO seeds solves the sludge volume problem also as it produces less amount of sludge for the same amount of removal in comparison to Alum.
Clinical manifestations, RWH, Reverse osmosis, Fluorosis, Nutritional prophylaxis, Antioxidants, TDS, Potash alum, MO, Polyelectrolyte, Coagulation
Fluorine is the 13th most abundant element on earth and is probably an essential element for animals and humans. It combines with other substances to form fluorides. Low concentrations provide protection against dental caries, especially in children. MCL of fluoride in potable water is approximately 0.5mg/L and is required to produce protective effects. Three main anthropogenic sources were identified as fertilizers, combusted coal and industrial waste with phosphate fertilizer being the most significance source of fluoride (Chouhan and Flora, 2010). Fluorides are ionisable and non-ionisable, organic and inorganic (Farooqui et al., 2008). Soluble organic fluorides, ingested through water and foods almost completely absorbed from the gastrointestinal (GI) tract by a process of simple diffusion (Maheshwari and Bansal, 2007). Ingested fluoride that is not absorbed into GI tract is excreted in the faeces. Some fluoride is also gets removed from the body through sweat. Ionic fluoride entering the acidic environment of stomach lumen gets largely converted into hydrogen fluoride (Whitford and Pashley, 2008). It’s rapidly distributed by the systemic circulation to the intercellular and extracellular sites of tissues (Maheshwari et al., 2007). However, ion normally accumulates only in calcified tissues such as bone and teeth. In blood F-ion is asymmetrically distributed between plasma and blood cells, so that the plasma concentration is approximately twice as high as that associated with the cells (Whitford, 1996). Fluoride is distributed from plasma to all tissues and organs. In humans and laboratory, approximately 99% of the total body burden of fluoride is retained in bones and teeth, with remaining distributed in highly vascularised soft tissues and the blood (Maheshwari, 2007a). Fluoride is concentrated to high levels within kidney tubules, so this organ has a higher concentration than plasma (Hamilton, 1990).
Clinical manifestations of fluoride toxicity
Fluoride predominantly affects the skeletal systems, teeth and also the structure and function of skeletal muscle, brain and spinal cord (Shashi et al., 1990). General symptoms of acute fluoride poisoning include non skeletal fluorosis viz. nausea, salivation, vomiting, diarrhoea and abdominal pain (Maheshwari, 2007b). Fluoride also alters the metabolism of some essential nutrients which leads to hyperlemia, hypocalcaemia, hypomagnesaemia, hypopophosphatemia. Persistent fluoride serum level leads to mineral homeostatic which ultimately causes cellular damage. Chronic fluoride toxicity occurs after the long-term ingestion of small amount of fluoride. It inhibits the synthesis of DNA, protein and inhibits cell proliferation and cytotoxic at the high doses (Kaminsky et al., 1990). Symptoms of long term of long term fluoride toxicity include emaciation, stiffness of joints, hyper salivation, tremors, tetanic contractions and abnormal teeth and bones. Other effects include lowered milk production and detrimental effects on reproduction. Fluoride is known to cross the blood brain barrier and accumulate in the brain of animals exposed to high fluoride levels (Vani and Reddy, 1988). Accumulation of fluoride in the hippocampus of the brain causes degeneration of neurons, decreases aerobic metabolism and altere free-radical metabolism in liver, kidney, and heart (Cicek et al., 2005). Long term exposure to fluoride leads to development of fluorosis, which is also known as a crippling and painful disease. Fluorosis includes skeletal, dental and non-skeletal fluorosis. Dental fluorosis occurs during the period of enamel formation and is linked to excessive incorporation of fluoride into dental enamel and dentine, which prevents normal maturation of enamel. Skeletal fluorosis includes inhibition of bone hardening (mineralization), causing the bones to become brittle and their tensile strength may be reduced (Grynpas, 1990). Symptoms include limited movement of joints, skeletal deformities, and intense calcification of ligaments, muscle wasting and neurological defects (Godfrey and Watson, 1988).
Mechanism of toxicity
Fluoride leads to toxicity as follows:
• Binds calcium ions and may lead to hypocalcemia which could further lead to osteoid formation.
• Disrupts oxidative phosphorylation, glycolysis, coagulation, and neurotransmission (by binding calcium).
• Inhibits Na+/K+-ATPase (Adenosine Tri Phosphotase), which could lead by hyperkalemia by extracellular release of potassium.
• Inhibits acetyl cholinesterase, which may be partly responsible for hyper salivation, vomiting and diarrhoea (cholinergic signs).
Exact mechanism of fluoride toxicity is not known. It has been suggested that oxidative stress can be a possible mechanism through which fluoride induces damage to the various tissue. Due to high electro negativity, fluoride ion (F-) has a proclivity to form strong hydrogen bonds, especially with –OH and-NH moieties in bio molecules. Fluoride is also able to exert powerful influences on various enzymes and endocrine gland functions that affect or control the status of oxidant/antioxidant systems in living organisms. Hydroxyl radicals (°OH) were previously proposed as initiation of lipid per oxidation (LPO) through iron catalyzed Fenton reaction in membranes (Halliwell and Gutteridge, 1986). The cell has several ways to alleviate the effects of oxidative stress, either by repairing the damage or by directly diminishing the occurrence of oxidative damage by means of enzymatic (SOD, Catalase, GPx, GR) and nonenzymatic antioxidants (GHS, vitamins and several essential micronutrients). Some studies have shown LPO as one of the molecular mechanisms involved in chronic fluoride-induced toxicity (Shivarajashankara et al., 2001). It may impair a variety of intra and extra mitochondrial membrane transport systems that may contribute to apoptosis. It leads to the formation of secondary products such as conjugated dienes, hydrocarbon gases (ethane), and carbonyl compounds (malondialdehyde) and decreased levels of poly unsaturated fatty acid (PUFA), Dexter et al., 1989. In addition to this ROS (reactive oxidative species) is also found to play major role during pathogenesis of fluoride. It may directly oxidize amino acids leading to a loss of function of proteins and a deactivation of enzymes (Stadman, 2001).
A possible mechanism of DNA damage induced by fluoride is as follows –
(a) Fluoride has a dense negative charge and is biochemically very active thus directly effect on DNA due to strong affinity for uracil and amide bonds by-NH...F-interactions (Li et al., 1987).
(b) Fluoride can combine stably with DNA by DNA;
(c) Fluoride can induce the production of free radicals, which can damage DNA strands directly or by LPO initiated by free radicals (Wang et al., 2004a); and
(d) Fluoride may depress enzymes activity, such as DNA polymerase which might further affect the process of DNA replication or repair and thereby damage DNA (Aardema and Tsutsui, 1995).
(e) Few studies have reported that fluoride does not induce DNA damage, while others have observed the genotoxic potential of fluoride in rats and human cells (Shanthakumari et al., 2004).
(f) Effect of fluoride on DNA damage in lymphocytes and its possible relation with oxidative stress needs extensive research. Fluoride was found to be an equivocal carcinogen by the National Cancer Institute Toxicological Program (Maurer et al., 1990).
(g) IARC (International Agency for Research on Cancer) evaluated that there is limited data, which provide inadequate evidence about fluori deinduced carcinogenicity.
(h) In a recent study, rats and mice given sodium fluoride (NaF) in drinking-water at 11, 45 or 79mg/ L have shown only the incidence of osteoporosis in bones of male rats (NTP, 1990).
Health education, treatment and prevention strategies
(i) Health Education
Creating awareness about the fluoride and fluorosis: the main area of interest will be
(a) Creating disease awareness: Creating awareness about the disease should be in the form of graphic presentation of the final consequences of the disease to the extent possible. If required, live presentations of the patients who are suffering from the severe form of the disease in areas where the gravity of the problem has not reached to that extent. It may be of use to demonstrate the most severe extent of the disease and to motivate them to use the preventive or therapeutic measures.
(b) Creating awareness about the sources of the fluoride: The creation of awareness will help in implementing the need based preventive measures in the affected community.
(ii) Treatment of the disease
Vitamin C and D, salts of Ca, Mg or Al were prescribed in an attempt to reverse these effects. Published results were, however, inconclusive and largely negative. Recent studies conducted in Rajasthan under Raj DST (Department of Science and Technology) sponsored studies indicated that fluorosis could be reversed, at least in children by a therapeutic regimen (Nutritional prophylaxis), which is cheap and easily available. The choice of the reported therapy was logical. The presence of calcium in gut directly affects the absorption of fluoride ions and also improves serum levels. Vitamin D3 in low doses enhances Ca absorption and retention without causing hypercalcemia and thus directly affects the absorption of fluoride ions. It also inhibits the excessive release of parathyroid hormone thereby preventing excessive activation of osteoblasts thus preventing hyperosteoidosis and osteopenia. Ascorbic acid controls collagen formation, maintains the teeth structure and bone formation. The structures are adversely affected by higher fluoride intake.
(iii) Preventive strtegies
(a) Providing defluoridated water for drinking purpose
Methods of defluoridation recommended so far are aimed at bringing the fluoride levels to the WHO standards. Desirable characteristics of defluoridation process, cost effectiveness, easy to handle, (operation by rural population) - the major sufferer - independent of input fluoride concentration alkalinity, pH, temperature, no effect on taste of water, no addition of other undesirable substances (e.g. Al salts) to treat water, all these parameters must be considered for adopting any of the defluoridation process/technique.
Commonly used domestic defluoridation processes
Fluorosis affects older persons, newborn baby and children of younger age. It not only affects the body of a person but also renders them socially and culturally crippled. Considerable work has been done all over the world on treatment of fluorosis. The effects of fluorosis are irreversible in children. A safe efficient and cost effective defluoridation technique/process needs to be developed in order to prevent the occurrence of fluorosis (Maheshwari et al., 2013b and 2013c).
Advantages and disadvantages of various commonly used processes available for defluoridation:
(1) Nalgonda Process
It looks a cumbersome technique not suitable for use by less educated population - the section that needs it the most. The process can be used only for water having a fluoride content of <10ppm & turbidity <1500ppm. There is a high residual Al content in output water. It is reported that the residual Al ranges from 2.01ppm to 6.80ppm. It is relevant to note that Al is a neurotoxin and concentration as low as 0.80ppm of Al in drinking water is reported to have caused Alzheimer’s disease. The ISO 10500 for drinking water sets an absolute max limit of 0.2ppm for Al, which is well below the minimum reported in the output water, generated by this process. Also the taste of output water is generally not acceptable.
After extensive testing of many materials and processes including activated alumina since 1961, National Environment Engineering Research Institute (NEERI), Nagpur evolved an economical and simple method for removal of fluoride which is referred to as Nalgonda Technique. Nalgonda Technique involves addition of aluminium salts, lime and bleaching powder followed by rapid mixing, flocculation, sedimentation, filtration and disinfection. Aluminium salt may be added as aluminium sulphate [Al2(SO4)3] or aluminium chloride (AlCl3) or combination of these two. Aluminium salt is only responsible for removal of fluoride from water. The dose of aluminium salt increases with increase in the fluoride and alkalinity levels, which are manipulated by adding lime, the raw water. The selection of either aluminium sulphate or aluminium chloride also depends on sulphate and chloride contents of the raw water to avoid them exceeding their permissible limits. The dose of lime is empirically 1/20th that of the dose of aluminium salt, but also depends on the alkalinity of water. Lime facilitates forming dense floc for rapid settling and also, neutralization of H+ ions released during the coagulation process. Bleaching powder is added to the raw water at the rate of 3 mg/L for disinfection#1
The chemical processes, though admittedly are not fully understood, can be seen below:
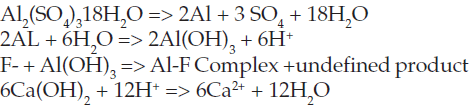
The amount of Al2(SO4)3 added must be carefully monitored as both left over aluminum can cause significant health problems including neurological, cardiovascular, and respiratory problems among others and must be kept under 0.2mg/L#2
There are limitations chemically as the Nalgonda Technique has been shown to not be sufficient for the treatment of water with a fluoride concentration greater than 10.0 mg/L. Also the pH is very difficult to regulate with the addition of lime and sludge created needs to be properly disposed of. The main problem of the Nalgonda Technique is the residual Aluminum in treated water which at times is found to be higher than the permissible limit, i.e. 0.2mg/L.
2) Activated Alumina Process
Reactivation of filter material is cumbersome and it can be done only with the help of trained persons generally not available in most of our villages. This process also results in high residual Al in output water ranging from 0.16ppm to 0.45ppm.

Table 1: Approximate Alum dose (mg/L) required to obtain acceptable quality (~1.0 mg/L) of drinking water from raw water at various alkalinity and fluoride levels#1 *To be treated after increasing the alkalinity with lime.
3) KRASS Process
This process differ from the known processes in its simplicity, cost effectiveness and only traces of residual Al in outlet water. There is no limit on fluoride concentration in input water. Temperature, pH, alkalinity and TDS of input water do not affect this process. It is a practical approach especially for our rural population. The importance of the process is a defluoridation process, which is easy to use by illiterate villagers, requires minimal involvement of technical personnel. In this process, once the filters are laid, the only expenditure is in terms of recharging with alum. This process have verified by CSIR (Council of Scientific and Industrial Research) and PHED (Public Health Engineering Department) of Rajasthan. The large scale, field installation KRASS’s plants is under process.
4) Other process
Processes like electro-dialysis, ion exchange and reverse-osmosis require special equipment, power, especially trained person to operate and require maintenance and are expensive.
Reverse Osmosis Technology
Membrane processes employ a semi-permeable (selective) membrane and a driving force (pressure difference, gradients in concentrations, electrical potential and/ or temperature) across the membrane to separate target constituents from a feed liquid. Different types of membrane processes can remove dissolved and colloidal constituents in the size range 0.0001 to 1 microns. The membrane has three layers. The first is a 500 to 2000 A polymer layer that does actual separation. The second layer is made up of porous polysulfone of 50 mm thickness. The third layer used for tear resistance and strength is made up of polyester with thickness of 125 mm. The membranes can withstand pH in the range 2-12 and temperature up to 60°C. One of the most important physicochemical criteria governing membrane separation of organic solute is the polar effect of the solute molecule which includes both the functional group and substituted groups for phenol and nitro-phenols. The commercially available membrane processes include, microfiltration. ultrafiltration, reverse osmosis, membrane electrodialysis and diffusion dialysis. Microfiltration and ultrafiltration are variations of CMF. In CMF, the fluid to be filtered flows parallel to the filtration surface that is, cross How with respect to the flow of the filtrate. The cross-flow generates shearing forces and turbulence across the filtration medium and limits the thickness of the particle deposits on the filtration surface. Because of the nature of flows within a tubular surface, a gradient in the particle concentration perpendicular to the surface is established. Microfiltration removes constituents between approximately 0.05 and 2 microns, while ultrafiltration removes constituents between approximately 0.005 micron and 0.1 microns. The disadvantages of membrane processes are high cost of equipment and difficulty with the separation of highly polar compounds (Maheshwari et al., 2013a).
The term "osmosis" describes the interaction between weakly concentrated aqueous solution and a more highly concentrated solution, separated by a semi permeable membrane. The membrane which is permeable to water molecules permits the diffusion of water from the lower concentration to higher concentration. If this natural process is reversed, say by raising the side with the higher concentration to a higher pressure, the flow of water will be in the opposite direction. Reverse Osmosis (RO) is thus a pressure driven membrane process used generally to remove constituents with molecular weights above 200. It lies become a common method for the treatment of household drinking water supplies. Effectiveness of RO units depends on initial levels of contamination and water pressure. The treatment may be used to reduce the levels of various contaminants as listed such as naturally occurring substances that cause water supplies to be unhealthy or unappealing (foul tastes, smells or colors) and substances that have contaminated the water supply resulting in possible adverse health effects. RO systems are typically used to reduce the levels of total dissolved solids including fluoride, nitrate and suspended matter. RO units with carbon filters may also reduce the level of some SOCs like pesticides, dioxins and VOCs like chloroform and petrochemicals.
Application of the process includes purification of water for use as make-up water, desalination of seawater, concentration of milk in the dairy industries, and dehydration of the liquid food. The separating capacity of the membrane is reliable. Salts and organic contaminants of groundwater can penetrate the membrane to a very small degree but the bacteria and viruses are incapable of penetrating it. Thus the reverse osmosis process is used as a reliable process for the production of extremely pure water. RO systems, normally used to treat only drinking and cooking water supplies, may not be preferred where larger supplies are being treated. It is possible to treat fluoride rich groundwater and make it safe for drinking purposes, using a sophisticated treatment plants (Which requires regular maintenance) based on reverse-osmosis-membrane technology. Out of various technologies available for defluoridation, reverse osmosis is probably the only most versatile and accepted technology today. Which offer the opportunity to provide the water quality standards as per the recommendations of WHO and EU specifications, practically from any source of raw water. It is a multistage process, in which water is forced through a semipermeable membrane of a pore size of 0.0001 micron, which rejects all undissolved and dissolved contaminants of groundwater including fluoride up to 98%. In Rajasthan people of number of towns and villages are being benefited by getting fluoride free water from RO systems.
(b) Changing the Dietary Habits
Defluoridation of drinking water alone shall not bring the fluoride level to safe limit. It would be necessary to overcome the toxic effects of the remaining fluoride ingested through other sources. This can be done by effecting minor changes in the diet and dietary habits of the population compatible with their social system and available resources. The main aim must be to
- Restrict use of fluoride rich food
- Avoiding use of fluoride rich cosmetics
- Use of food rich in Calcium, Vitamin C and anti oxidants
There is no safe and effective treatment for the cases of chronic fluoride toxicity. However, the treatment for acute poisoning mainly relies on the use of antioxidants, vitamins and essential elements. Administration of some vitamins like vitamin C and E known to revert toxic effects induced by fluoride exposure. The mechanism of action of vitamin C might be due to its powerful reducing action (Chinoy, 2002). During fluoride toxicity, generated free radicals attack the double bonds of PUFAs initiating a chain reaction and affect membrane integrity and cellular function. This chain reaction is inhibited by vitamin E (α- tocopherol) by reacting with free radicals and converting itself into an α-tocopheroxyl radical which is not harmful (Nair et al., 2004). This α-tocopherol radical, thus formed is converted back to α-tocopherol by cytosolic vitamin C (Basu et al., 1996). Thus vitamin C and E show synergistic action in the recovery of altered variables suggestive of oxidative stress and organ damage by fluoride exposure. In addition to this certain non-vitamin antioxidants such as Coenzyme Q (Co-Q) and liponate have also been studies against fluoride toxicity. CoQ is present in cells in two forms: oxygenated (ubiquinone) and a reduced form (ubiqunol). Only the reduced from demonstrates antioxidative properties. It reduces the concentration of MDA in rabbit blood plasma, wherein it prevents the initiation and propagation of proxidation of PUFAs, lipids and phospholipids of mitochondrial membranes (Czeczot, 2002). Grucka-Mamczar et al., 2009, have studied the effect of some vitamin (A, C, and E) and non-vitamin antioxidants (Coenzyme Q and liponate) on fluoride induced lipid peroxidation and found that antioxidants are most effective in counteracting the free radical processes generated by NaF.
Flavanoids like quercetin has also been studied against fluoride poisoning which support its beneficial role on lipid peroxidation, serum cholesterol level, triglycerides and total proteins in fluoride intoxication (Czerny et al., 2000). Mixture of quercetin sulphonates has been reported to stimulate and normalize tissue respiratory activity and thus, can be useful for the prevention of fluoride toxicity in persons who are exposed to excessive fluoride (Juzyszyn et al., 2002). Combination of vitamin C and E has been reported to protect endometrial tissue via their antioxidant function on fluoride-induced damage (Guney et al., 2007). As such there is no effective treatment of fluorosis. Therefore, prevention and control is the only approach to manage the menace. It is known that a nutritionally rich diet may play an important role in alleviating fluoride intoxication. It has been reported that supplementation of adequate dietary factors such as protein, calcium (Ca), magnesium (Mg), melatonin and selenium (Se) may significantly reduce toxic effects fluoride in bone and other tissues (Wang et al., 2004b). These substances decrease the absorption of fluoride and increase its removal from the body. Aluminium promotes the urinary excretion of fluoride, calcium and phosphate interfere the gastrointestinal absorption of fluoride and borate enhances its elimination process (Yao and Wang, 1988).
In people with exposure and those with clinical and sub clinical symptoms, the only available measure as of today is eliminating the intake of fluorides. No chemical till date is capable of extracting fluoride absorbed in the body. In patients with disease symptoms, the following interventions should be practiced:
(a) Reduce as much as possible the fluoride through water and food.
(b) Practice consumption of diet rich in calcium, vitamin C (ascorbic acid), vitamin E and anti-oxidants.
A properly designed nutritional regimen can beneficially interfere with the toxic effects of fluoride. Vitamin C, vitamin E and anti-oxidants, which are beneficial and are not very expensive, can be produced in rural areas without much investment.
a. Calcium : Milk, Curd, Yoghurt, Green leafy vegetables, Jaggery, Drumstick, Sesameseeds
b. Vitamin C : Aaonla, Lemon, Orange, Tomato, Sprouted cereals/pulses and Dhania leaves
c. Vitamin E : Vegetable oil, Cumin seeds, Nuts, White grain cereals, Green vegetables and Dried beans
d. Anti-oxidants : Garlic, Ginger, Carrot, White onion, Papaya, Pumpkin and Green leafy vegetables. All the above items have antagonistic effect; thereby play the prophylactic role in preventing fluorosis.
(c) Rain Water Harvesting: (Alternative water source)
Fluoride affects the people and the animals as well. Therefore it is desirable that the animals should also be provided with fluoride free water for maintaining their longevity. Defluoridation of drinking water for animals will be too costly and not feasible and thereforethe only solution of this problem is water harvesting. The water harvesting technology should be aimed not only to provide fluoride free water to human beings but also to animals. Rainwater storage can be a major source of fluoride free drinking water for the animals. These three-pronged attacks can prove to be a blessing for the population especially for the younger generation living in fluoride rich areas having no choice except to drink the water contaminated with fluoride and suffer the inevitable consequences including permanent deformities.
To Defluoridate Groundwater Employing Moringa olefera Seeds and Potash Alum
Moringa oleifera (MO) is a multipurpose, medium or small-sized tree, from regions of north- west India and indigenous to many parts of Asia, Africa, and South America. Its pods have been employed as an inexpensive and effective sorbent for the removal of organics, and coagulant for water treatment. It is a non-toxic natural organic polymer. MO is a tropical plant belonging to the family Moringaceae, a single family of shrubs with 14 known species. MO is native to India but is now found throughout the tropics. It is a nontoxic natural organic polymer. The tree is generally known in the developing world as a vegetable, a medicinal plant, and a source of vegetable oil. It is drought tolerant and has nutritional, medi- cinal, and water-cleaning attributes. Its leaves, flowers, fruits, and roots are used locally as food articles. The medicinal and therapeutic properties of this plant have led to its application as a cure for different ailments and diseases, physiological disorders, and in eastern allopathic medicine (Vieira et al., 2010). The powdered seed of the plant MO has coagulating properties that have been used for various aspects of water treatment such as turbidity, alkalinity, total dissolved solids and hardness. However, its bio-sorption behavior for the removal of toxic metals from water bodies has not been given adequate attention (Kumari et al., 2005). Purification of artificially fluoridated waterdone by Bazanella et al., 2012, at a starting fluoride concentration of 10 mgL-1by submitting it to a coagulation process with aqueous extracts of M. oleifera seeds. The coagulation process was followed by ultrafiltration with membranes at different pressures. The coagulation process with 2.5 gL-1 of M. oleifera promoted a reduction of 90.90 % in the fluoride content of the treated water, making it possible for poor communities to consume this water. For their method, the combined coagulation/filtration process using raw coagulant showed the highest values of colour and turbidity, which, however, were still below the limits set for drinking water by Brazilian legislation.
An active component of MO was used by Ghebremichael and Hultman, 2004 in comparison with synthetic polymers and alum for the conditioning of chemical sludge from a drinking water treatment plant. The comparison was based on dewatering characteristics of the conditioned sludge determined by capillary suction time (CST), specific resistance to filtration (SRF), sand column drainage and shear strength tests. The results indicated that MO showed comparable conditioning effect as alum. Polyelectrolytes were more effective than MO and alum. Sludge conditioned with MO and alum, as in dual chemical conditioning, showed better results than MO alone. According to CST, SRF and sand drainage results, optimum doses for MO, alum and polyelectrolytes were 125, 63, and 1.8 kg/t, respectively. Comparison of the twopolyelectrolytes showed that the cationic polyelectrolyte was more effective. For sand drainage tests both polyelectrolytes improved the drainage rate by 2orders of magnitude. MO and alum improved the drainage rate by about 4.2 times. On the other hand, the improvements in cake solids concentration were similar for all the chemical conditioners. Flocs from MO and alum were relatively stronger compared to those of the polyelectrolytes. From the results of the study it could be concluded that MO alone or in combination could be effectively used and replace alum for dewatering of chemical sludge.
The triumph in the fluoride and fluorosis mitigation achieved through persistent and consistent effects spanning over a period of 2 decades by scientists. From a variety of disciplines including the water sector and biomedical sciences across the country have made the proud. It is no small an achievement. It is the desire of very Indian that let the success achieved in the fluoride and fluorosis front be a model for those involved in dealing with other contaminants like nitrate, salinity, arsenic, heavy metals and pesticides, to be pursue a path, resulting in unquestionable victory. Several years of fundamental research on fluoride action on animal and human body tissues at the cellular and molecular levels generated a wealth of information and knowledge. The path breaking discoveries emerged through unconventional approach adopted for multidisciplinary investigations of both soft and hard tissues were a revelation. The true disease characteristics emerged, tend to early diagnostic procedures for the disease. Differential diagnoses of fluorosis from other disease with overlapping clinical manifestations become necessary. Simple tests with focus on assessing that poison levels in body fluids provided meaningful information. No sooner the disease could be correctly diagnosed at very early stages, it become necessary to eliminate / reduce the poison levels in the body fluids, leading to disappearance of health complaints that are non-responding to medication. What are the health complaints which are referred to?
First and foremost gastrointestinal discomfort with pain, constipation, nausea and loss of appetite should never be dismissed as casual. Low haemoglobin content (< 9 g/dl) should alert. Anaemia, depression, fatigue and muscle weakness are health complaints overlooked. It is equally important to be aware of excess thirst (polydipsia) and tendency to urinate more frequently (polyurea) can also be due to fluoride interfering with hormonal production which has adverse effects on kidney function. If any of the above health complaints is confirmed to be closed by fluoride poisoning require no medication except for practice of interventions. Withdrawal of the source (s) of fluoride entry to the body results in arrest of the progression of the disease and health complaints referred to above shall cease to exist. However, if speedy recovery is the aim, yet another intervention i.e. diet enriched by essential nutrients along with micro minerals (Zn, Cu, Mg and Se) besides vitamin C and E, and other antioxidants need to be promoted through fruits and vegetables. An enriched diet insures repair and maintenance of the damaged parts of the body, rise in haemoglobin and total recovery of the disease.
It is a new era for practice of integrated disease management. A patient of fluorosis if diagnosed correctly and early by the consulting physician and if the source of fluoride entry is through drinking water, then the responsibility lies on the Water Supply Agency to guide/advise and direct the patient as to now to obtain ‘safe water’ for consumption. The intervention procedure dealing with enriched diet with nutrients and antioxidants shall be dealt with by the consulting physician. Monitoring the patient for complete recovery and assessing the impact of the practice of the interventions shall be of the responsibility of the hospital or the physician dealing with the patient. The Water Supply Agency (ies), till date have never practiced nor is aware how a patient is going to look-upon to the Public Health Engineer(s) for quality water for getting rid of the disease after obtaining the diagnosis of the disease from a physician. The present practice of indiscriminate supply of defluoridated water to the community leaving in an endemic area may not relieve those who are afflicted with fluorosis, as the fluoride entry to the body may be much more from the sources other than drinking water.
From experiments employing Moringa oleifera (MO) seed and potach alum it can be inferred that MO seeds can be tried to be used in tandem with alum in the Nalgonda Technique, which can lead to aluminum free treated water and less sludge generation. Also, as we know it is not possible to treat water having fluoride level above 10ppm by Nalgonda Technique, hence, MO seeds can be used at the start where there is fluoride level above 10ppm to bring down the fluoride level as much as possible to below 10ppm, and then use alum to reduce the level further. And once the level is lowered by MO seeds, the amount of Alum required to reduce further will be less, and hence, less chances of high residual concentration of Aluminum being found in treated water. MO seeds can be used alone, but it has been seen generally that it does not reduce well at low concentrations.
Copyright © 2024 Research and Reviews, All Rights Reserved